




Editor's note: This is the second segment in a two-part article.
Obstetric-related lawsuits
While lawsuits against medical practitioners are not the same as criminal charges against them, lawsuits could still be an indicator of medical performance.
Have lawsuits for obstetric-related reasons changed post-Dobbs? The answers could shine some light on changes in doctors’ actions and patient/family expectations of medical treatment when pregnancy is involved.
Unfortunately, most of the information I was finding on obstetric-related medical malpractice lawsuits was limited to lawyer websites and did not give me the granular details I wanted to find.
Instead, I looked at the raw data from the National Practitioner Databank (NPDB) myself, which is what most websites were citing as their source material.
The NPDB “is a web-based repository of reports containing information on medical malpractice payments and certain adverse actions related to health care practitioners, providers, and suppliers.” The raw data is available for public download.
Because 2025 is not yet over, I have not included 2025 numbers in anything below. I went back to 2016 to cover both pre- and post-Dobbs and different sitting presidents. When I say “payout(s)” I am referring specifically to payouts for obstetric-related medical malpractice lawsuits.
What do we find?
- The COVID-19 pandemic had the opposite effect on payouts as it did on MMR.
I first found that overall, payouts statistically significantly dipped when actual MMR increased in 2020 and 2021. In 2022, the number of payouts returned to within the normal range for pre-pandemic years.
However, in 2023 and 2024, payouts have statistically significantly increased (Figures 1 and 2). In 2020 and 2021, economic impacts of the pandemic may have led to the significant decrease in malpractice payouts. If people couldn’t afford legal fees to file a claim in the first place, then fewer payouts would be the result. But why the uptick in the past couple of years? Are pro-life states contributing the most to that increase?
Figure 1: Bar chart of payouts per year.
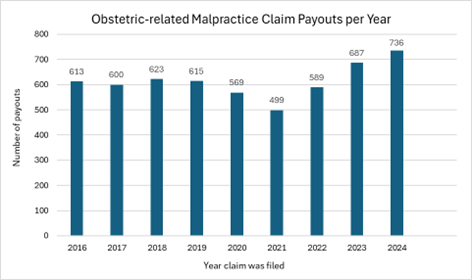
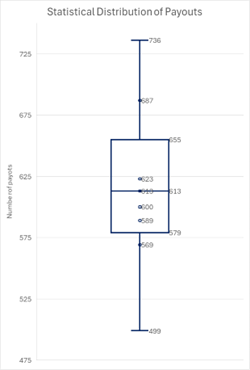
Figure 2: Quartile analysis of payouts since 2016 using a box and whisker chart. Data points above and below the boxes (part of the “whiskers”) are statistical outliers to the data group.
[Click here to subscribe to Pregnancy Help News!]
2. Overall, a higher population means more payouts, but abortion restrictions specifically do not seem to have a controlling effect on the number of payouts.
California, the most populous state, has had the highest number of payouts since 2016. Texas, the next most populous state, has the fourth-most payouts. And Florida, which is the third most populous state, has the second-most payouts. So, generally, the more patients in a state, the more malpractice claims get filed, and the more payouts are awarded — though this correlation is not exactly direct.
Let’s compare two abortion states with hundreds of payouts since 2016, California and New Jersey.
While the population of California is over four times that of New Jersey, there have only been 1.3 times as many payouts in California (396) compared to New Jersey (316). California, while very much an abortion state, has more limits on abortion than New Jersey does.
If what abortion activists suspect is true, the more abortion limits there are, the more at risk a pregnant woman’s health is. However, even though California is much more populous than New Jersey and has more abortion restrictions, the number of malpractice payouts is not as much higher as one would expect.
If we compare two abortion states with much more similar abortion laws and populations, we still see differences in malpractice payouts. The populations for New Jersey and Michigan are much more similar, with Michigan’s population only 1.06 times that of New Jersey’s. Both Michigan and New Jersey have no gestational limits on abortion … but New Jersey still has two times as many malpractice payouts (316) as Michigan does (154).
When we look at life states, Texas is about 1.3 times as populous as Florida and is more restrictive about abortion; but Florida has 1.4 times as many malpractice payouts (368) compared to Texas (254). Here, the less restrictive, less populous state had more payouts.
If we look at California compared to Texas, California is 1.2 times as populous as Texas and has much fewer abortion restrictions, and has 1.6 times as many malpractice payouts (396) as Texas (254). Here, the malpractice payouts increased more than the population increase alone may account for, and the suspected protective factor of being a more pro-choice state does not seem to be true.
3. The severity of the injury on the payout claim is not necessarily correlated to abortion legislation.
Comparing four abortion-friendly states and four pro-life states, there is no clear-cut association between abortion legislation and severity of the claims.
For the four abortion states, I chose the top three most populous ones that have no gestational limit (New Jersey, Maryland, Michigan) and the most populous one overall that has a very generous gestational limit of fetal viability (California).
For the four pro-life states, I chose the top two most populous ones that have total elective abortion bans (Texas, Indiana) and then the next two most populous ones that have the next-strictest set of laws with a 6-week LMP ban (Florida, Georgia).
Type of injury ranged from only emotional injury to death. The worse the injury, the higher the number of payouts, which makes sense. The worse the injury, the more likely the patient or their family are to seek restitution and the more likely they would be to win. The top three injuries listed were, order of most common to least common: Death (1471); quadriplegic, brain dead, or lifelong care (1144); and major permanent injury (1082).
I looked at these most listed injuries for all eight states, comparing only these injuries for the female patient who was the mother, not including these injuries which were listed for the unborn or born child.
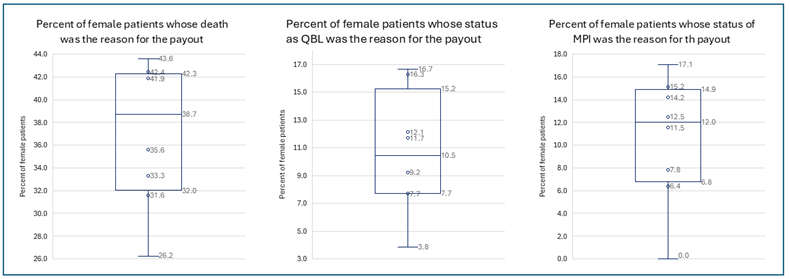
No single life or abortion state had a statistically significantly higher or lower percentage across all three injury types. There was no pattern in general for the statistically different percentages, either — both life and abortion states could be outliers in either the positive or negative direction (Table 2, Figure 3).
Table 2: The number of payouts for varying levels of severity of the claim by state. QBL means quadriplegic, brain dead, or lifelong care. MPI means major permanent injury.
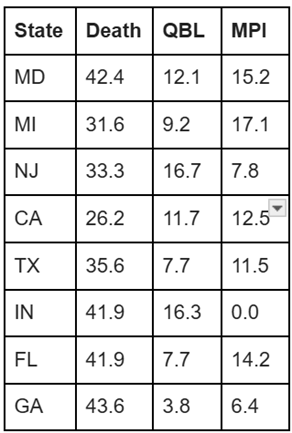
Figure 3: Quartile analysis of payouts since 2016 by severity and state using a box and whisker chart. Data points above and below the boxes (part of the “whiskers”) are statistical outliers to the data group. The data is all in Table 2.
Are doctors also activists?
The American Medical Association (AMA) has a list of principles for medical ethics that places the patient first.
However, doctors are also called to be advocates or activists: “A physician shall respect the law and also recognize a responsibility to seek changes in those requirements which are contrary to the best interests of the patient.”
In a 2022 paper publication in the New England Journal of Medicine, a different AMA quote is noted:
“In some cases, the law mandates conduct that is ethically unacceptable. When physicians believe a law violates ethical values or is unjust they should work to change the law. In exceptional circumstances of unjust laws, ethical responsibilities should supersede legal duties.”
Doctors are already being called to civil disobedience of state abortion restrictions or bans.
This ethical principle is not bad in and of itself. However, it does help give some insight as to why we often see abortion supporting doctors arguing that abortion regulations interfere with necessary care and that they will refer for or prescribe abortion pills even illegally.
In an NPR article from November 2022, the author discusses the debate in the medical community between doing elective or “medically necessary” abortions and staying away from abortion or anything that could possibly be construed as an abortion. It describes in great detail the general fear, panic, and anger that abortion supportive doctors have. The only quotes from abortion affirming doctors it includes, though, are from those who provide elective abortions; it only hypothetically touches on abortions or abortion procedures that would be within the law to provide due to a legal medical exception.
According to the article, even five months after the release of Dobbs and 13 states had enacted abortion restrictions or bans, “leading medical associations tell NPR they aren't aware of any health care workers who have actually been charged with providing an abortion in violation of these new state laws.”
The article also quotes UC Davis Law Professor Mary Ziegler:
“The country has settled into an ‘uneasy reality,’ she says, where doctors aren't providing abortions in places where it's illegal — including in some emergency situations where abortion is technically allowed under the new restrictive legislation — and prosecutors aren't bringing charges.”
The admissions here are that doctors are indeed letting fear reign. There is so far no evidence to support their fears. Not a single doctor, pre-Roe or post-Roe, has been criminally convicted of violating a state’s abortion ban when acting on behalf of the health or life of the pregnant woman.
The article did offer some balance, as well:
“‘My perspective is that interpreting life and health exceptions to be consistent with standard medical practice is not lawbreaking,’ she [Katie Watson, bioethicist and professor of law and humanities at Northwestern University Feinberg School of Medicine] says. Those laws are generally intended to block elective abortions, and most have exceptions for medical emergencies. Plus, the federal government requires hospitals to stabilize patients, including when they need abortion procedures.
She acknowledges the legal risks and stiff penalties clinicians face, but says they need to better understand the legal protections they do have.”
Dr. Matthew Wynia is quoted heavily throughout the article. He is a doctor and a bioethicist and worked at the AMA for 18 years. He specifically mentions that he wants doctors “to follow the standard of care for a patient, even when that may violate state abortion laws” and “Strong leadership at the institutional level could embolden doctors to follow their medical judgment and cause fewer instances of doctors delaying care to consult legal experts.”
The irony here is that state abortion laws do let doctors use their judgment and standard of care to decide if an abortion is necessary.
Conclusion
While doctors may actually be fearful of messing up and going to jail for saving a woman’s life, the fears are based more on anxiety of the unknown than any evidence or precedent.
Tweet This: While doctors may be fearful of abortion laws, the fears are based more on anxiety of the unknown than any evidence or precedent.
Additionally, the fears are being stoked by pro-abortion doctors, ethicists, organizations, and media, who are claiming the medical profession is in danger and jail time is a looming, imminent threat to normal standard of care.
As Dr. Ingrid Skopp, a pro-life OB-GYN with over 30 years of experience points out, abortion supportive medical organizations could be helping their doctor members with clarity regarding the laws; instead, they are staying silent or merely emphasizing changing the law or breaking the law if needed. She argues persuasively that this silence and emphasis on not clarifying legal language for doctors seems to be intentionally sowing misinformation amongst doctors and allowing women to be harmed “in pursuit of political and ideologic goals.”
In fact, sometimes this goal is explicitly mentioned.
Take, for instance, what the chief legal officer for the very abortion affirmative American College of Obstetricians and Gynecologists (ACOG) says is wrong about abortion bans with medical necessity exceptions:
“The problem with these clarifying laws is they don’t expand access under the law, they don’t change the definitions, and they don’t remove the legislative interference in the practice of medicine.” [emphasis added]
Notice her very first issue with exception language, even when clarified extensively as Texas did, is simply that abortion access is not expanded.
In reality, the laws are not made to prosecute doctors. They are made to stop elective abortions.
It all smells more like a campaign to simply get elective abortion made legal throughout pregnancy with no exceptions, ever, than it has anything to do with making sure women get care when problems happen during pregnancy.
Editor's note: Heartbeat International manages Pregnancy Help News. Views expressed by authors external to Heartbeat International are their own and may not necessarily represent those of Heartbeat International or Pregnancy Help News. This is the second segment in a two-part article.



